
Thyroid Anatomy
 Fig.1: Thyroid position in the neck in front of the trachea (windpipe)The thyroid is a gland that sits across the windpipe like a bow tie, just below the Adam's Apple. It has a shape a bit like a butterfly, with the thyroid lobes forming the wings and the isthmus the body of the butterfly (Fig. 1).
Fig.1: Thyroid position in the neck in front of the trachea (windpipe)The thyroid is a gland that sits across the windpipe like a bow tie, just below the Adam's Apple. It has a shape a bit like a butterfly, with the thyroid lobes forming the wings and the isthmus the body of the butterfly (Fig. 1).
The isthmus usually lies over the second and third tracheal rings opposite the fifth, sixth and seventh cervical vertebrae. The lobes of the thyroid are almost always asymmetrical with the right lobe larger than the left. The weight of the thyroid is approximately 20-25 grams but the size of the gland varies with the amount of iodine in the diet.
The thyroid is surrounded by a sheath that binds the thyroid to the larynx and the trachea, which is why it moves up when swallowing. It is also attached to the trachea by a suspensory ligament (Berry's ligament), first described by Berry in 1888.
The strap muscles sternohyoid and sternothyroid lie in front of each of the lobes. A pyramidal lobe is also often present and it projects upwards from the isthmus as seen in the diagram. A fibrous or muscular band frequently connects the pyramidal lobe to the hyoid bone, reflecting the embryological origin of the gland.
 Fig.2: Tubercle of Zuckerkandl overlying the recurrent laryngeal nerve
Fig.2: Tubercle of Zuckerkandl overlying the recurrent laryngeal nerve
The Tubercles of Zuckerkandl
During embryological development of the thyroid (see an overview of the embryology origins here), there are lateral contributions on either side that fuse with the median component, and in adult life these become the Tubercles of Zuckerkandl. These were first described by Emil Zuckerkandl in Vienna in 1902 and occur in around 55% of patients to a more or lesser degree.
The posteriorly-placed Tubercle of Zuckerkandl plays an important role in thyroid surgery. It is of variable size, from a hugely expanded mass down to just a small tongue of tissue, wrapped around the recurrent nerve and often extending behind the trachea and oesophagus. The growth of this part of the thyroid can press on the oesophagus leading to dysphagia (swallowing difficulty). Thus it needs to be identified and removed during thyroid surgery, to prevent it becoming a source of persistent unrelieved symptoms or recurrence.
An understanding of the anatomy of the Tubercle of Zuckerkandl is also central to safe surgical dissection, particularly its close relationship to both the recurrent laryngeal nerve and the superior parathyroid (Fig. 2).
The tubercle usually enlarges lateral to the recurrent laryngeal nerve, with the nerve appearing to pass into a cleft medial to it – this is the situation in 93% where the nerve is deep to the Tubercle. Early elevation of the tubercle of Zuckerkandl usually allows the recurrent nerve to be easily and safely “encountered” even though not initially visible.
However an uncommon (7%) but high risk situation is where the recurrent laryngeal nerve runs lateral to an enlarged Tubercle of Zuckerkandl, placing it at increased risk of damage during dissection.
Another important point is that the normal superior parathyroid gland, also being derived from the 4th branchial cleft, is commonly found in close association, superior to the Tubercle of Zuckerkandl (see below for further description of the ligament of Berry).
 Fig.3: Blood supply of the thyroid, showing major vessels and surrounding structuresThe Blood Supply
Fig.3: Blood supply of the thyroid, showing major vessels and surrounding structuresThe Blood Supply
The thyroid is richly supplied with blood vessels, with a blood supply almost twice as rich as that of the kidney. When the thyroid is very large, the massive blood flow to the gland is audible as a noise (bruit). There are three main arteries supplying the thyroid gland:
- Superior thyroid artery
- Inferior thyroid artery
- Thyroidea ima artery
The major blood supply to the thyroid is from the paired superior and inferior thyroid arteries. The superior thyroid is a branch of the external carotid artery and enters the thyroid at the upper poles of each lobe. The artery is also accompanied by the external laryngeal nerve.
The inferior thyroid artery is a branch of the thyrocervical trunk and it runs behind the gland to the level of the cricoid cartilage. It then turns medially and downwards to supply the posterior of the gland. A lower thyroid artery (the thyroidea ima) may arise from the brachiocephalic artery or from the arch of the aorta, and climbs up to the thyroid in front of the trachea. There is also a troublesome small artery (the inferior laryngeal artery) close to the ligament of Berry and the RLN.
All the arteries anastomose with each other over the surface of the gland (Fig. 3).
There are three main veins draining the thyroid gland:
- Superior thyroid vein
- Middle thyroid vein
- Inferior thyroid vein
The superior and middle thyroid veins drain into the internal jugular vein. The inferior thyroid veins anastomose with each other and drain into the left brachiocephalic vein in the thorax.
The parathyroid glands are usually found at the posterolateral borders of the thyroid lobes and in 80% of cases, their blood supply is via the inferior thyroid artery. The position and number of parathyroid glands is variable, although four is the most common.
The Recurrent Laryngeal Nerve
The recurrent laryngeal nerve (RLN) runs either in front of or behind the 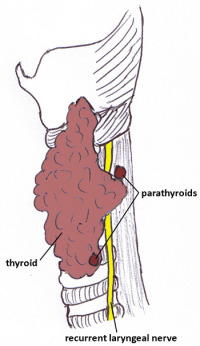 Fig.4: Left side view of RLN positioninferior thyroid artery and it is essential to locate this nerve during a thyroidectomy. It was Lahey, a doyen of thyroid surgery, who suggested that careful dissection of the nerve would definitively decrease the number of injuries.
Fig.4: Left side view of RLN positioninferior thyroid artery and it is essential to locate this nerve during a thyroidectomy. It was Lahey, a doyen of thyroid surgery, who suggested that careful dissection of the nerve would definitively decrease the number of injuries.
The nerve is paired and arises from the vagus. It supplies all the muscles of the larynx (except the cricothyroid) and is the major nerve supply of the vocal cords.
On the right hand side, the nerve passes behind the vagus and loops under the subclavian artery, tending to have a more angled, lateral position (and is thus more at risk of injury during thyroidectomy). On the left, the nerve passes under the arch of the aorta and tends to ascend more vertically, in the tracheo-oesophageal groove.
The nerves then pass beneath the tubercles of Zuckerkandl, and the superficial vascular layer of Berry's ligament, and enter the larynx under the inferior constrictor (Fig. 4).
Non-recurrent Laryngeal Nerve
The recurrent laryngeal nerve can be 'non-recurrent' on the right in less than 1% of cases, opening it up to potential injury during thyroid surgery. A non-recurrent right laryngeal nerve (nRLN) is associated with an arterial anatomical abnormality.
The embryological abnormality is arteria lusoria, in which the fourth right aortic arch is abnormally absorbed. This results in the right subclavian artery arising directly from the aortic arch, passing up in a retro-oesophageal position, with the nerve therefore not pulled down to the usual position in the neck.
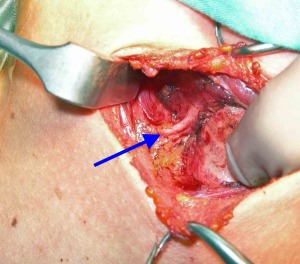 Fig.5: Non-recurrent laryngeal nerve following course from lateral side towards larynx. Finger is retracting the trachea medially.
Fig.5: Non-recurrent laryngeal nerve following course from lateral side towards larynx. Finger is retracting the trachea medially.
When the nerve is not found in the classic position at thyroid surgery, a non-recurrent nerve should be suspected.
The non-recurrent nerve will tend to follow a transverse path parallel to (and either over or under) the trunk of the inferior thyroid artery, or between its branches (Fig. 5). This makes a nRLN particularly vulnerable at ligation of these vessels.
A left non-recurrent laryngeal nerve is only possible with a right-sided aorta, found in situs inversus, so is extremely rare.
RLN Bifurcation
The RLN can bifurcate outside the larynx (usually in the last 2cm of its course) in around 20-25% of patients, more commonly on the right side. Up to 5% will have bilateral branched RLNs. In addition, if the nerve is bifid on the left side, then 40% will also be bifid on the right.
It is important to realise this fact as work done by Prof Serpell has shown that the anterior branch (the smaller of the two) carries the motor fibres. The RLN carries 55% motor fibres and 45% sensory, but the distal nerve tends to be about 80% motor, as sensory nerves branch off on the way up the neck. Adductor fibres outnumber abductor fibres in a ratio of 3:1, so after damage, the return of function tends to be adductor first.
There is a risk of presuming that the larger posterior branch represents the whole of the nerve, thus potentially putting the motor fibres in the anterior branch at risk. Having a bifid RLN does increase the risk of injury, emphasising the importance of completely dissecting the nerve, rather than assuming it is safe.
Berry's ligament
Work in the Monash Endocrine Surgery Unit has also shown that there are 2 fascial layers enveloping the RLN: a superficial vascular layer and the deeper, 'true' Berry's ligament. The superficial fascial layer (which contains the superior parathyroid, and the tubercle of Zuckerkandl) must be divided to reveal the RLN, which lies in the groove under the tubercle, lateral to the true ligament of Berry.
Once the true ligament of Berry is divided, the lobe springs forward and the RLN (pulled forward into a genu by traction) relaxes backward and becomes serpiginous again. There is often an annoying small vessel (the inferior laryngeal artery) that needs to be divided close to the ligament of Berry, or it will produce troublesome bleeding right in the danger zone for the RLN.
The External Branch of SLN
The external branch of the superior laryngeal nerve (EBSLN), and often called just the superior laryngeal nerve, is a further nerve supply to the larynx that is in danger during thyroid surgery.
It is a small nerve branch that innervates the cricothyroid muscles and in particular the cricoarytenoid muscles of the larynx, which tighten the vocal cords to allow high pitched sounds. It also facilitates explosive sounds and shouting, and is very important in those who use their voice professionally.
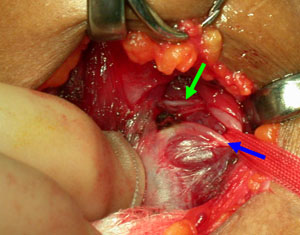 Fig.6: External branch of SLN (green arrow) and its close relationship to the superior thyroid artery (blue arrow)It lies in close proximity to the superior pole of the thyroid (and the superior thyroid vessels) in variable position and has a number of anatomical variations that can put it in danger during dissection of the thyroid (Fig. 6).
Fig.6: External branch of SLN (green arrow) and its close relationship to the superior thyroid artery (blue arrow)It lies in close proximity to the superior pole of the thyroid (and the superior thyroid vessels) in variable position and has a number of anatomical variations that can put it in danger during dissection of the thyroid (Fig. 6).
These have been classified by Cernea into 3 variants, according to their relationship to the superior thyroid vessels and pole (Fig. 7). Type 1 is most common (and safest), where the nerve crosses the superior vessels more than 1cm above the superior thyroid pole.
Type 2a is the more dangerous for the voice, occurring in about 35% of cases. This is where the EBSLN crosses the pedicle less than 1cm above the superior thyroid pole, and so is in danger during ligation of the vessels, particularly in surgery for large goitres. The worst variant is Type 2b, where the nerve crosses the vessels below the superior thyroid pole (occurring in 20% of cases).
 Fig.7: Cernea classification of the anatomy of the External Branch of the Superior Laryngeal Nerve
Fig.7: Cernea classification of the anatomy of the External Branch of the Superior Laryngeal Nerve