
Conn's Syndrome (Hyperaldosteronism)
 Fig.1: Jerome ConnPrimary hyperaldosteronism was first described by Jerome Conn in 1954, and his findings published in 1955 (Fig. 1). The collection of clinical and biochemical abnormalities is commonly called Conn's syndrome. The syndrome results from an abnormally large amount of aldosterone being produced from the adrenal cortex. The excess production of aldosterone will result in the retention of sodium, and thus increased water retention, which leads to the main clinical finding in Conn's syndrome of hypertension (high blood pressure).
Fig.1: Jerome ConnPrimary hyperaldosteronism was first described by Jerome Conn in 1954, and his findings published in 1955 (Fig. 1). The collection of clinical and biochemical abnormalities is commonly called Conn's syndrome. The syndrome results from an abnormally large amount of aldosterone being produced from the adrenal cortex. The excess production of aldosterone will result in the retention of sodium, and thus increased water retention, which leads to the main clinical finding in Conn's syndrome of hypertension (high blood pressure).
Secondary hyperaldosteronism occurs when abnormally large amounts of aldosterone are produced by the adrenals due to increased renin activity (e.g. in pregnancy or chronic heart failure).
Incidence
Primary hyperaldosteronism was originally thought to occur in 1% of people diagnosed with hypertension, back in the days when low potassium levels in the blood were required for diagnosis. More recent work suggests that the majority of Conn's patients in fact have normal potassium levels, so the prevalence was probably underestimated. The use of the aldosterone/renin ratio as a screening test has also led to an increase in detection.
It appears that the real prevalence of Conn's syndrome may actually be between 5-13% of hypertensive patients, and as much as 20% in those with resistant hypertension, although this is debated. Conn's is twice as common in women as in men and its incidence is highest in persons aged between 30 and 50 years.
Causes
Aldosterone-producing adrenal adenomas (aldosteronoma)
These benign tumours account for 65% of adult cases. They are usually found in only one adrenal gland, are between 0.5cm and 2.5cm in diameter, and typically they are golden yellow in cross-section (Fig. 2).
 Fig.2: Histology section of a typical adrenal Conn's adenoma (left) and cross-section of adenoma in adrenal specimen showing typical golden yellow appearanceThey are normally unresponsive to angiotensin II, but still retain some responses to ACTH. As in all tumours a genetic cause is suspected.
Fig.2: Histology section of a typical adrenal Conn's adenoma (left) and cross-section of adenoma in adrenal specimen showing typical golden yellow appearanceThey are normally unresponsive to angiotensin II, but still retain some responses to ACTH. As in all tumours a genetic cause is suspected.
Idiopathic hyperaldosteronism (bilateral adrenal hyperplasia)
This is the most common cause of primary hyperaldosteronism in children and in 30% of adult cases, but the underlying cause is unknown.
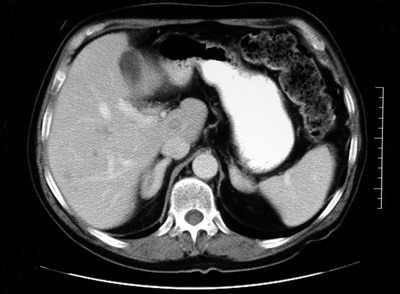 Fig.3: CT scan showing bilateral adrenal hyperplasiaThe adrenal glands start to grow excessively to produce nodules, either large (macronodular) or small (micronodular) that secrete aldosterone (Fig. 3). These seem to be responsive to angiotensin II, but not ACTH.
Fig.3: CT scan showing bilateral adrenal hyperplasiaThe adrenal glands start to grow excessively to produce nodules, either large (macronodular) or small (micronodular) that secrete aldosterone (Fig. 3). These seem to be responsive to angiotensin II, but not ACTH.
These pathological features are not absolute however, as it is not uncommon to find adenomas with surrounding hyperplasia. Thus the pathological changes represent a spectrum of disease.
Other causes
The remaining 5% of cases are due to:
- aldosterone-secreting adrenocortical carcinomas (malignant tumours of the adrenal cortex)
- unilateral adrenal hyperplasia
- familial hyperaldosteronism type I (glucocorticoid-suppressible aldosteronism or GSA)
- familial hyperaldosteronism type II (familial aldosteronoma)
Presentation
Hypertension (high blood pressure) due to retention of sodium and water by the kidney. This is moderate to severe, and refractory to medical treatment. It is often asymptomatic, but can cause headaches.
Note that the absence of hypertension makes the diagnosis of hyperaldosteronism most unlikely.
Hypokalaemia (loss of potassium) symptoms tend to be non-specific, but can include thirst with polydipsia (excessive drinking), polyuria (increased frequency of urination) and nocturia (excessive need to urinate at night). Other possible symptoms are: muscle weakness, paraesthesia (partial loss of sensation of parts of the body) and cramps.
Cardiac & metabolic alterations including increased risk of heart attack and stroke, and insulin resistance, causing diabetes.
Next page: Conn's Syndrome diagnosis